
2 min read
Context
Sturge-Weber syndrome is a condition usually diagnosed in childhood.
This article reports the unusual case of a 61-year-old man with no prior neurological history who developed severe epileptic seizures known as status epilepticus.
These episodes were prolonged, difficult to control, and led to temporary neurological deficits such as weakness on one side of the body.
Brain imaging (MRI) revealed a leptomeningeal angioma, a vascular malformation located on the surface of the brain.
This type of lesion is typically associated with Sturge-Weber syndrome.
Why it matters
This case is notable because:
- The patient had no classical features of the syndrome (no facial birthmark, no ocular involvement)
- Symptoms appeared late in adulthood, which is highly unusual
What we found
Imaging showed focal hypoperfusion and localized cortical atrophy.
Histological findings revealed vascular abnormalities.
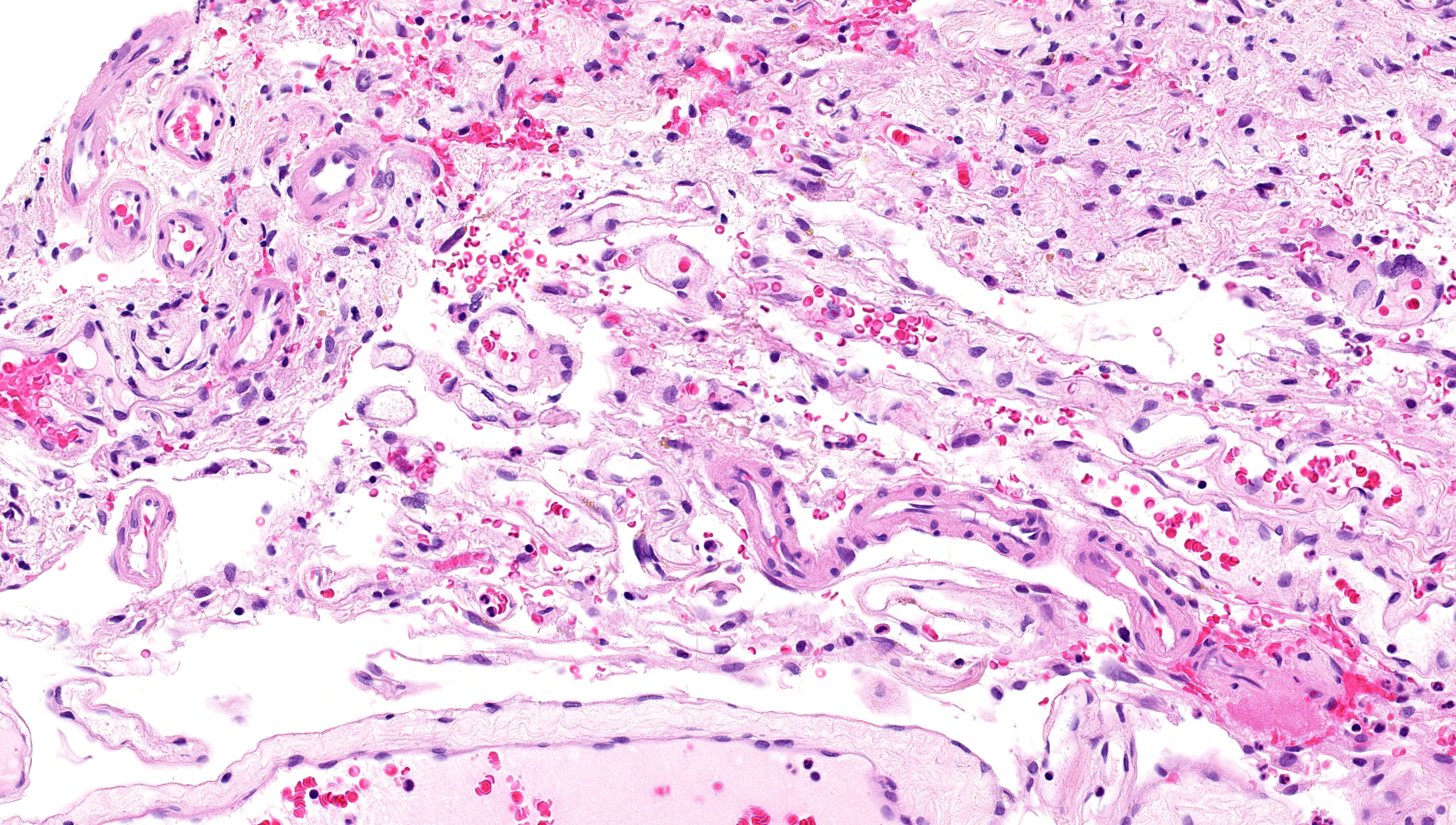
Leptomeningeal vascular abnormalities
Enlarged veins with angiomatosis.
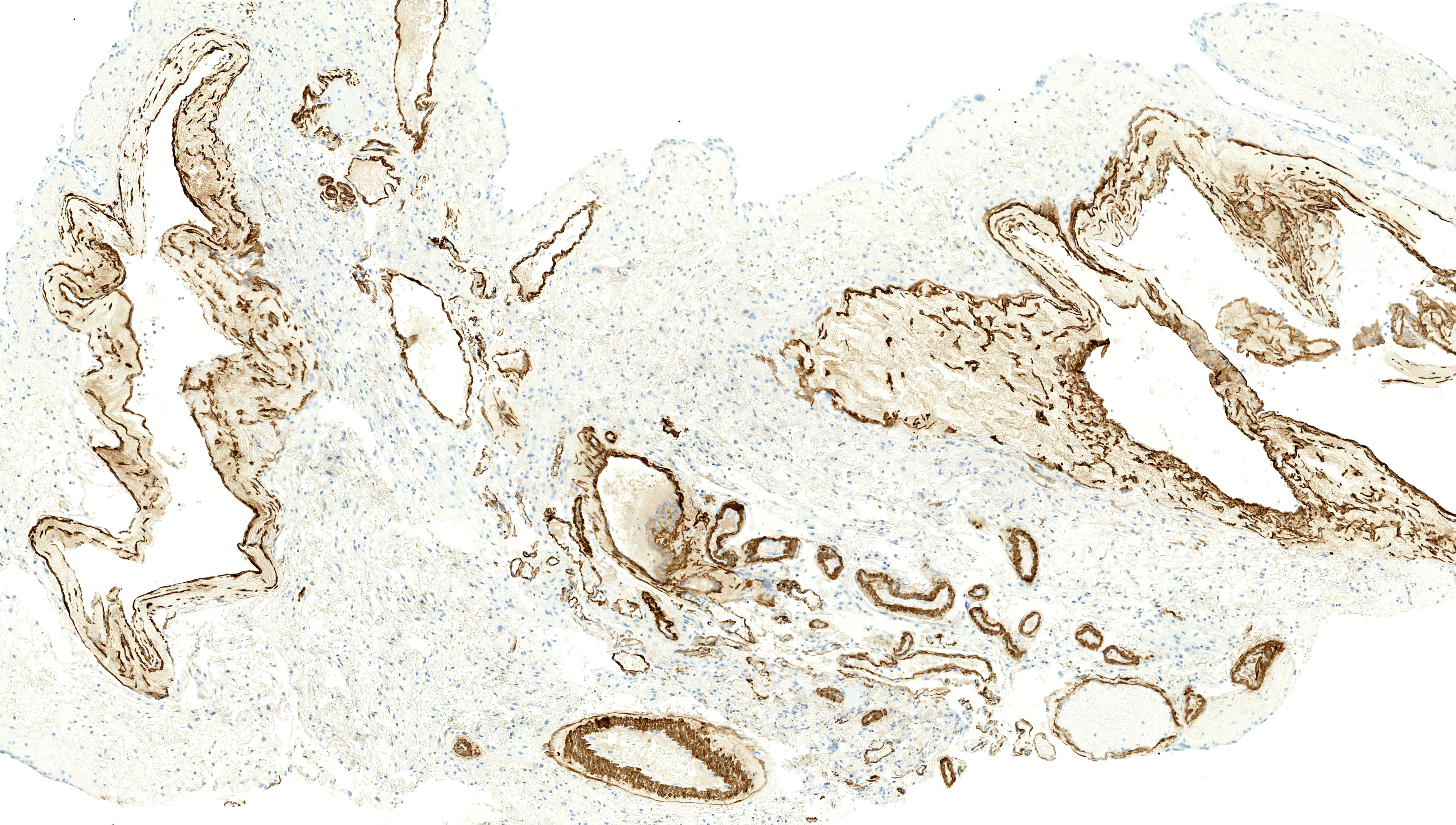
Abnormal smooth muscle actin expression
Abnormally expressed alpha-smooth muscle actin in vein wall.
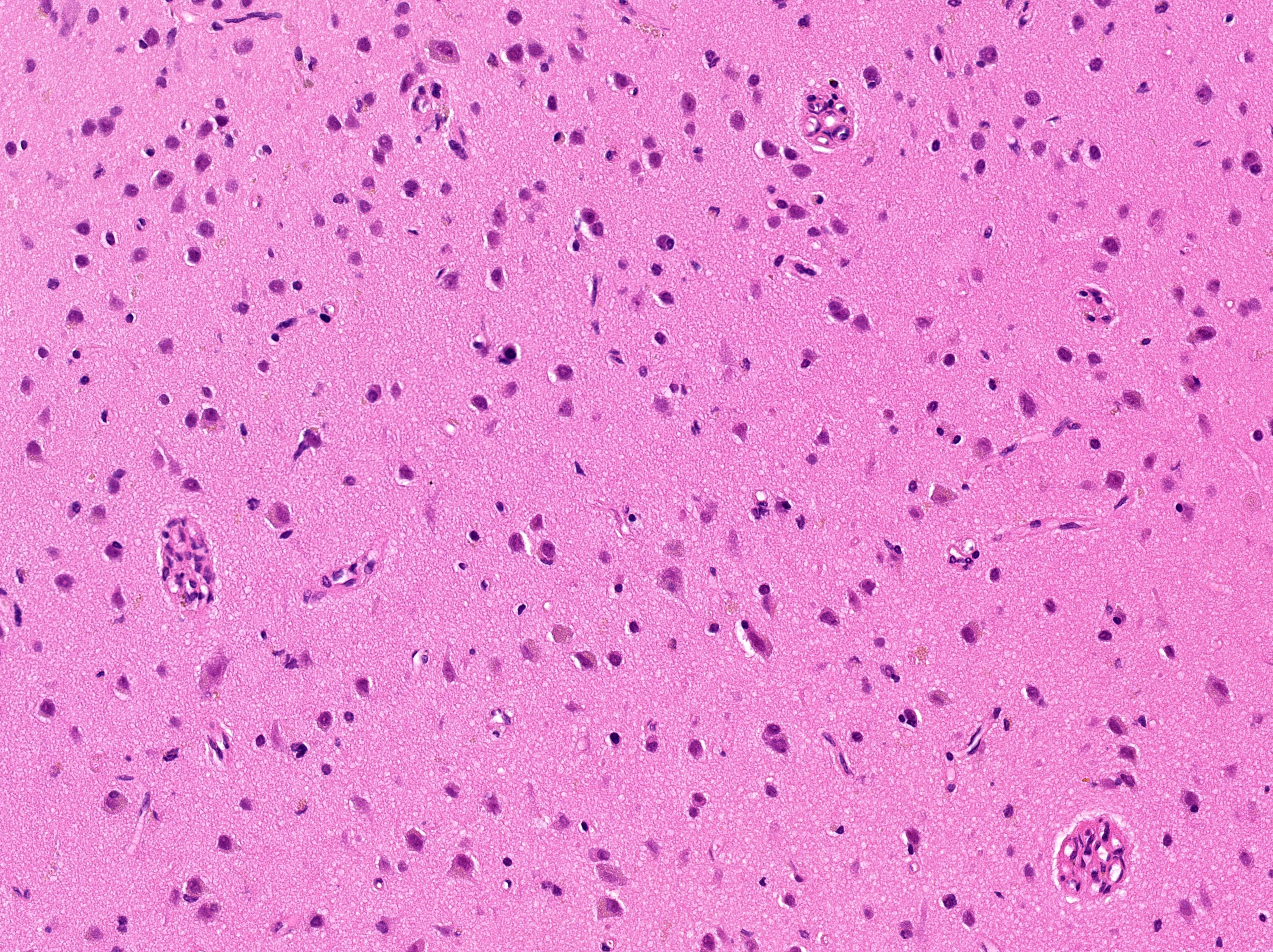
Cortical glomeruloid vessels
Cortex (layers II–III): glomeruloid vessels without neuronal loss, gliosis, or calcification (×200–400).
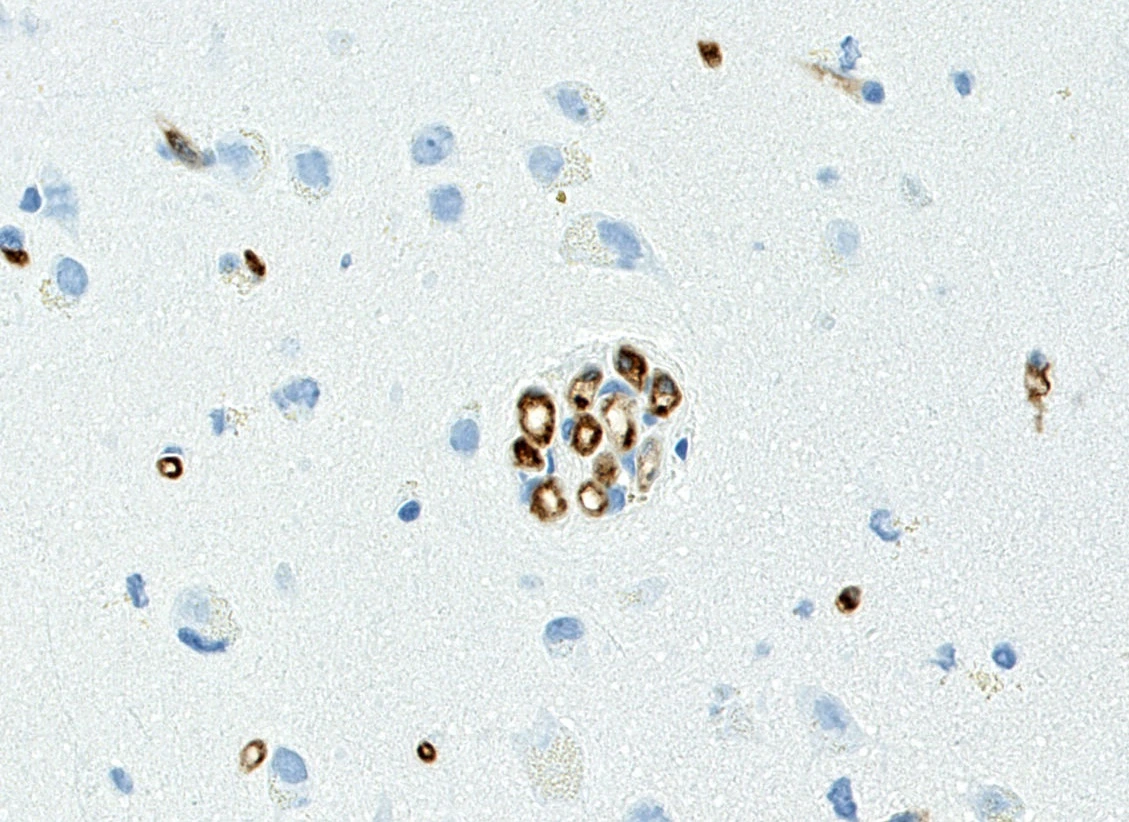
CD34 endothelial staining
CD34 staining of the glomeruloid vessels.
On the leptomeningeal biopsy, we identified a specific somatic mutation GNA11 R183C (VAF: 4%), previously known to be involved in Sturge-Weber syndrome.
Together, these findings support the diagnosis of type III Sturge-Weber syndrome.
Contribution to knowledge
This case shows that:
- Sturge-Weber syndrome can exist without the full set of signs and symptoms
- It can manifest later in life as severe epilepsy
- It reinforces the role of genetic mutations, particularly somatic mutations, in these atypical forms
In practice, this suggests that some unexplained adult-onset epilepsies may have an underlying, underdiagnosed vascular-genetic origin.
Other publications

Histogenetic Classification Predicts Outcomes in 130 Adults With Chronic Intestinal Pseudo-Obstruction
Integrating genomic and histopathological data resolved 82% of idiopathic cases. Monogenic myopathy emerged as an independent predictor of favorable long-term survival.

Insights into the expanding intestinal phenotypic spectrum of SOCS1 haploinsufficiency and therapeutic options
SOCS1 haploinsufficiency can cause severe intestinal diseases, including Crohn's disease and chronic intestinal pseudo-obstruction.

NR1D1::MAML3 Fusion in an Aggressive Mesenchymal Neoplasm
NR1D1-rearranged tumors are emerging aggressive mesenchymal neoplasms.

PFMG2025-integrating genomic medicine into the national healthcare system in France
The 2025 French Genomic Medicine Initiative represents one of the first nationwide efforts to integrate whole genome sequencing into routine clinical care.